

The Menopause Paradox
Why menopause is everywhere—except the practice of medicine

When was the last time you read or heard something that struck such a chord, you couldn’t stop thinking or talking about it for days?
That’s how I felt listening to Dr. Rachel Rubin—a urologist and sexual medicine expert—in conversation with Dr. Peter Attia on his podcast, The Drive, as they unpacked the completely abysmal state of menopause care in America.
It wasn’t that the information was particularly new to me—I’ve spent a decade in women’s health and am well versed in the long shadows cast by the notorious Women’s Health Initiative (WHI). But the way they spoke about the scale of the damage—not just for patients, but for providers—hit differently.
“The WHI is the greatest injustice imposed by the modern medical system in our lifetime.” — Dr. Peter Attia
This kind of no-BS truth-telling from two world-class physician researchers set me off on a quest to make sense of the question that wouldn’t let go:
If menopause is so “hot”, why are so few women getting the care they need and deserve?
The answer lies in what I call The Menopause Paradox—the gap between growing cultural awareness, rising consumer demand, and a clinical workforce that’s been left behind.
Cultural Zeitgeist > Clinical Zeitgeist
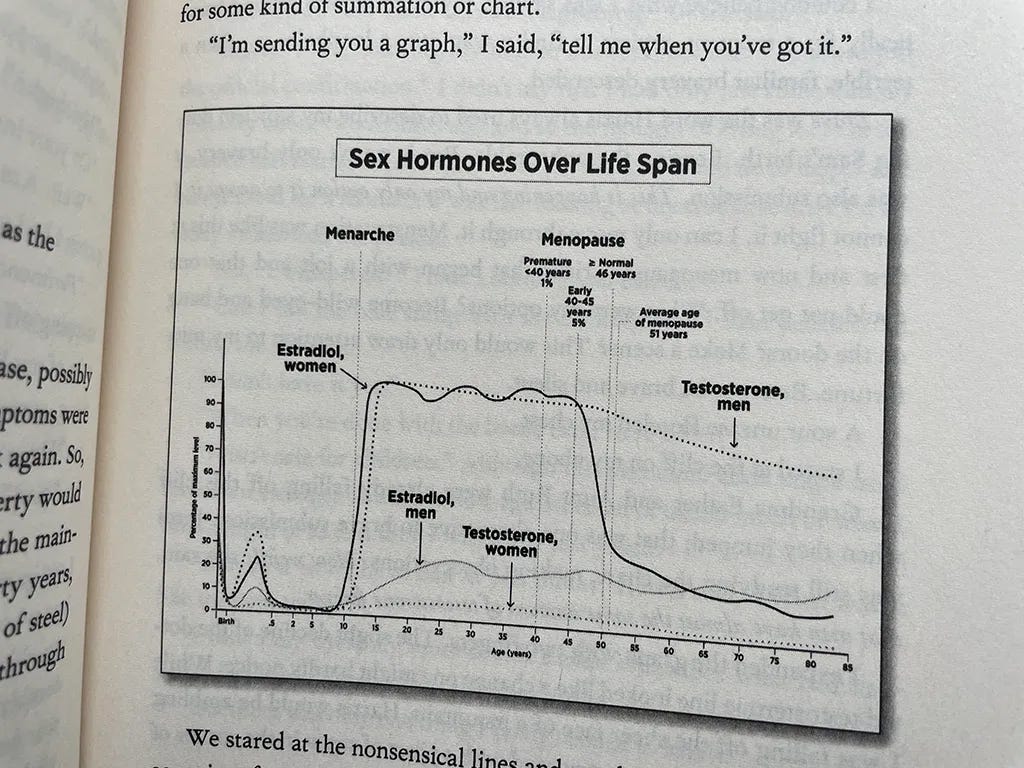
Yes, menopause is having a moment. It’s on Oprah. In The New Yorker. In Miranda July’s buzzy novel, All Fours. Who could forget the viral “hormonal cliff” graph?
Menopause is the subject of one of the few bipartisan bills in Congress. And every celebrity—from Gwyneth Paltrow to Michelle Obama to Halle Berry—is helping break the taboo by sharing her own menopause story (and increasingly, launching a wellness brand to go with it).
Today, it’s hard to imagine being a woman aged 35 to 55 and not having at least some baseline knowledge of menopause, and the possibility of hormone replacement therapy (HRT) as a potential solution.
And yet… fewer than 4% of U.S. women are on HRT—down from nearly 40% before the WHI. How is this possible?!
The Lost Generation of Menopause Providers
The problem isn’t patient demand—women are showing up at their doctor’s office, asking for help, and increasingly, for hormones. The real bottleneck is clinical expertise. While menopause dominates the cultural conversation, few clinicians are actually trained to treat it, due to what Dr. Rubin describes as a generational “brain drain” in clinical knowledge:
“This is a disaster…. It’s not enough to say the WHI was misinterpreted; providers don’t know how to do this. The doctors who prescribed HRT either retired or died and there was no one they taught ahead of them... We are now trying to make up for lost time to train people how to write prescriptions.” — Dr. Rachel Rubin
I saw this dynamic play out with my own mom.
She is one of the lucky ones amongst women of her generation—cared for by an incredible OB/GYN who is a true hormone expert and early debunker of the WHI. Thanks to her, my mom was educated on and prescribed HRT during perimenopause, and reaped the many health benefits as a result.
But when that doctor recently retired, her new provider tried to take her off hormones cold turkey—a move we now know can halt and even reverse many of the long-term brain, bone, and cardiovascular benefits of HRT.
Well versed in the latest evidence, I was able to step in, advocate for my mom, and get her access to hormone therapy elsewhere. But it left me wondering: what happens to everyone else?
Solving the Menopause Paradox
If we want to unknot this knot—to make quality, menopause care mainstream not just culturally, but clinically—we need to treat The Menopause Paradox like the public health crisis it is.
Yes, more patient education is needed. Women deserve clear, evidence-based information about the safety and efficacy of HRT—especially in a world awash with misinformation, wellness influencers, and lingering WHI-era fear.
But even more importantly, we need to invest upstream—in the systems that shape what clinicians are taught and how care is delivered to expand access to high quality menopause care at scale.
Tactically, that means:
Redesigning medical school so that every provider is trained in menopause as an integral part of their speciality and whole-body medicine
Backing purpose-built menopause clinics (not pill mills!) expanding access responsibly
Using AI to augment clinicians—a 1+1=3 multiplier for solving quality and access gaps at scale
#1: Redesigning medical school
Menopause is the orphan child of modern medicine. It affects 50% of the population and nearly every system in a woman’s body, yet is claimed by no speciality. As Dr. Rubin so astutely puts it:
“Menopause medicine is the tiniest little room of subset of gynecology—it should not be under gynecology—this is whole body medicine!” — Dr. Rachel Rubin
Without a clinical home, it’s no wonder that the majority of providers—including OB/GYNs—receive less than one hour of formal menopause training during medical school. And why fewer than 10% of providers feel equipped to treat menopause or prescribe HRT today.
To fix this, we need to stop siloing menopause as a reproductive issue defined by the end of your period. Hormonal shifts in midlife affect everything—women’s brains, hearts, bones, sleep, and skin. Every specialty—from cardiology to orthopedics to neurology—should be trained to understand how hormones intersect with their field.
Better yet, we should create a dedicated women’s health residency. You can go to medical school to specialize in geriatric medicine and pediatric medicine; why not women’s medicine?
#2: Backing purpose-built menopause clinics
Recognizing the vast clinical gap in menopause care and the market opportunity that comes with it, there’s been a boom in startups competing for women in midlife. But not all next-gen disruptors are created equal. To be blunt, there’s a lot of snake oil out there.
As much as I support expanding access to HRT, the growing presence of “pill mill” models gives me pause. With large compounding players entering this space—often with perverse incentives to prescribe broadly—we risk reducing menopause care to what Midi CEO, Joanna Strober, calls a “vending machine” for hormones. Let’s just say, that’s not the appropriate solution to the problem.
Listen to Dr. Rubin describe the full toolbox of options—from systemic estrogen to oral progesterone, testosterone and beyond—and you’ll quickly see why prescribing hormones is not an Advil vs. Tylenol decision. Quality menopause care requires robust counseling, dialogue and ongoing titration—not a 3 minute quiz with a clinician “rubber stamp” on the backend.
Thankfully, a new wave of purpose-built menopause clinics show us how to fill the gaps in care responsibly—with novel care models that prioritize both quality and access. To understand what best-in-class care looks like, I spoke with the Chief Medical Officers of Midi, Elektra Health, and Tia (yes, I acknowledge I have a horse in this race!). Most importantly, I’d trust all three of these companies to care for my own mother. A few themes stood out:
Training must be continuous—not one and done
When it comes to menopause care, credentials and tenure aren’t enough. Providers must be continuously trained to make up for what they didn’t learn in medical school and to keep pace with the rapidly-evolving body of evidence.
Elektra addresses this by hiring providers certified by The Menopause Society—the leading authority on evidence-based menopause management in the U.S. The challenge? There are only ~3,000 certified providers nationwide, and tens of millions of women of peri/menopause age who need care.
Recognizing these supply-side limitations, Midi and Tia have made substantial investments to close this training gap themselves. They’ve each developed in-house training programs that blend live instruction, asynchronous learning, patient case studies, and assessments. These programs are designed to up-level new hires—including those with no prior experience in menopause care.
Importantly, training doesn’t stop once a provider starts seeing patients. At all three clinics, ongoing education is baked into clinical operations and provider workflows.
As Dr. Kathleen Jordan, Chief Medical Officer of Midi, puts it:
“With medical knowledge doubling every 72 days, we need information and training support to be dynamic—continuously refreshing clinicians on up-to-date knowledge and really as close to real time as possible.” — Dr. Kathleen Jordan
At Midi, continuous learning includes weekly clinical updates, Loom videos with “clinical pearls,” and chart-scrubbing AI that flags outdated practices and triggers targeted retraining.
Tia takes a similar approach to keeping clinical knowledge both current and actionable. As Jess Horwitz, Chief Clinical Officer at Tia, explains:
“We recognize that we’re learning more every day about how best to care for women in midlife, and that national guidelines don’t always reflect best-in-class care. To address this, we’ve built our own systems to keep Tia's internal protocols and resources updated with the latest research and recommendations—leveraging AI to surface relevant protocols and trainings to providers directly in the portal.” — Jess Horwitz, MSN FNP-C
In short, the best menopause clinics treat training not as a checkbox, but as a core differentiator—baked into both onboarding and the day-to-day delivery of care.
Quality menopause care requires a multidisciplinary lens
As discussed, menopause is not limited to a woman’s reproductive organs; so the providers delivering menopause care shouldn’t be limited to OB/GYNs either.
All three players intentionally hire beyond traditional specialties, pulling from family medicine, internal medicine, and other disciplines. What unites their teams isn’t a specific speciality, but a shared commitment to whole-person, evidence-based care.
“High quality menopause care starts with listening to women—listening to how they feel, what is concerning them, what their goals are, and what they are scared about. From there, we design a patient’s care plan, which may include hormone replacement therapy, but also heart health and longevity, mental health, GLP-1s for metabolic health and acupuncture to support her sleep.” — Jess Horwitz, MSN FNP-C
Midi’s model is similarly interdisciplinary—aimed at solving the conflicting specialist problem many patients deal with. Each Midi clinician is trained and supported by a team that brings together multiple specialties so patients don’t have to reconcile guidance from four different doctors.
This team-based, multidisciplinary approach is one of the biggest distinctions between holistic, purpose-built menopause clinics and those in the business of writing and refilling prescriptions. Great care takes time, nuance, and collaboration—not just a script on demand.
A love of learning matters more than the letters after your name
Just as clinical specialty isn’t the most important determinant of quality menopause care, neither are credentials.
Across Tia, Midi, and Elektra, care teams include a mix of MDs, nurse practitioners (NPs), and physician assistants (PAs)—a reflection of the growing understanding that great menopause care comes from rigorous training and clinical curiosity, not necessarily a single degree.
As Dr. Nora Lansen, Chief Medical Officer at Elektra Health, explains:
"MD vs NP is not relevant...An NP trained and certified in menopause management is just as competent in this domain as a physician who is menopause trained and certified." — Dr. Nora Lansen
At Midi, mindset similarly matters more than background. According to Dr. Jordan:
“Our best clinicians are lifelong learners. If they have a few years of clinical experience, facilitating the right education and ongoing learning is what they need to be experts.” — Dr. Kathleen Jordan
In sum, it’s not about the letters after someone’s name—it’s about identifying, training, and supporting providers who are committed to learning and evolving with the science.
#3: Using AI to augment clinicians
If most clinicians aren’t yet equipped to deliver high-quality menopause care… is AI?
If I could wave a magic wand and clone Dr. Rubin to provide menopause care for every woman, I would. But that’s not an option. And while next-gen clinics like Midi, Tia, and Elektra are expanding access every day, scaling high-touch, team-based care to every woman who needs it is no small feat either. We should be doing everything we can to resource and replicate these models—but we also need additional levers.
Curious to assess how ready AI really is for this challenge, I recently tested ChatGPT for its menopause counseling capabilities. I expected little more than a generic HRT explainer, but was pleasantly surprised by the depth of information, personalization and emotional intelligence (dare I say “bedside manner”?) of the experience.
Beyond the obvious speed and real-time information advantages, here’s what stood out (for those interested, you can read my full ChatGPT patient simulation here):
It validated my experience and made me feel heard
It asked personalized, values-based questions (e.g. what matters to you? what’s bothering you most right now?)
It explained things in plain-English, without dumbing it down
It took a personalized, all-options approach to HRT—explaining how different forms and types of hormones might help different symptoms, and various risk factors to consider for each
Was it perfect? No. I found the biggest gap to be credibility and actionability. How could I know if the information was accurate and trustworthy? And, of course, ChatGPT couldn’t actually prescribe hormones or monitor how I was doing over time (at least not yet).
But here’s the thing: for most women today, the standard menopause visit doesn’t check those boxes either. Many women leave their appointments feeling dismissed or under-informed—still unsure what their options are, how to weigh the risks and benefits, and how to get hormones if their doctor refuses to prescribe them.
When I shared my ChatGPT transcript with a few doctor friends, they too were wowed. As Dr. Ajay Haryani, founder of primary care practice, Seen Medical told me:
“If I was assessing a clinician and witnessed this conversation, I would be generally impressed.” — Dr. Ajay Haryani
Regulatory aside, generalized AI is not comprehensive enough yet to prescribe, but it’s getting us 85% of the way there in terms of risk identification and education—and is frankly more in-depth than what most women are receiving today in the traditional system.
Given how quickly AI is improving relative to the slow pace of medical education reform, it’s easy to imagine how—with some minor tinkering or a purpose-built model—this technology could “unknot the knot” and solve The Menopause Paradox at scale.
Beyond co-pilots: AI-enabled collaborative care
While we may be years away from a fully autonomous “AI doctor” (at least from a regulatory and reimbursement standpoint), the opportunity for AI + clinician collaboration in menopause care is already here.
Tools like AI co-pilots and clinical decision support systems can help providers keep up with the ever-expanding medical evidence base—solving the “chasing your tail” problem that Dr. Jordan alluded to. Patients, too, are rapidly adopting tools like ChatGPT and Claude pre and post doctor’s appointments—to know what questions to ask, make sense of lab results, and research treatment options.
From my vantage point, we’re still in the early innings. The biggest opportunity lies in a fundamentally new interaction model—one where patients and providers don’t use AI separately, but together.
Imagine this: your rushed, transactional appointment transforms into a dynamic, three-way working session. Rather than an invisible AI silently transcribing in the background, it becomes an active, visible participant in the visit—available to both patient and provider. It pulls up your labs and benchmarks them against women your age. It fields real-time research queries using the latest and greatest evidence, and synthesizes disparate symptoms, lab results, and clinical notes from across specialist visits—surfacing relevant insights in seconds.
You and your clinician review the data together. You both ask questions, weigh tradeoffs, and co-create a care plan—with the AI offering context, not commands. After the visit, the AI doesn’t disappear. It stays with you: helping you implement your plan, track progress, stay accountable, and loops in your provider as needed to make timely adjustments.
In this model, there’s no illusion that the doctor knows everything—or that they should have to. Instead, all three parties engage in a transparent dialogue: the AI supports clinical reasoning, the clinician interprets and guides using frameworks rather than relying on rote recall, and you—the patient—are empowered to make decisions with clarity and confidence.
The result? Care feels more human and credible. Decisions feel more informed and thought through. And trust is built not on encyclopedic knowledge, but on shared understanding and collaborative sensemaking.
This, to me, is the real unlock: not AI instead of clinicians, but AI with clinicians and patients together—forming a whole new type of care team. This is patient-centered care, 3.0.
Bringing the pieces together
Menopause is finally mainstream—receiving the long-overdue cultural attention it deserves. But without matching clinical progress, it risks becoming a hollow victory.
Awareness alone isn’t enough. Not when millions of women are left navigating a broken system, forced to choose between clinicians who lack adequate training and hormone “vending machines” that prioritize prescription volume over quality of care. Not when providers themselves are asking for better training and smarter tools to help them deliver the kind of patient-centered, evidence-based care that drew them to medicine in the first place.
Solving The Menopause Paradox at scale requires multiple levers. Some must be aimed at fixing legacy systems, like outdated medical education. Others must be geared towards the future—leveraging generative AI to create new tools and models of care that don’t even exist yet.
With over 1 billion women worldwide in peri/menopause, the opportunity is gigantic. There is no silver bullet, but there is a clear path forward.
By shifting menopause from a cultural movement to a clinical one, we can close the training gap, scale new models of care that pair quality with access, and help more women in midlife get the holistic menopause care they need and deserve.
If you’re new here, The XX Factor is a curated dose of insights, analysis and conversation shaping the future of women’s health. My goal is to spark questions, challenge assumptions, and foster connections that help us all build smarter, faster, and with greater impact.
To learn more about why I started this, check out my first post introducing The XX Factor here—and some of my most popular deep dive pieces on maternity policy, the growth-stage cliff plaguing women’s health, and why every company is becoming a “women’s health” company.
Such a great post! I hear over and over "I'm just glad menopause finally has so much awareness" - and in some ways, we've accepted that that's enough. But you're right: there's a gap that exists before awareness can actually translate into meaningful change in care.
This is an incredibly insightful article with an excellent future state recommendation. Great thinking Carolyn!