



A "Baby Bonus" Won’t Save Mothers
Instead, let’s seize the political interest to fix the system.


One of my favorite things to do when traveling abroad is to talk to women about their health experiences. Across cultures and continents, a simple question like, “how do you find being a mom?" often opens the floodgates. From fertility journeys to birth stories, epidural debates to postpartum struggles, I find most women are waiting for an invitation to share—to candidly connect (and occasionally commiserate!) on the full, complex terrain of womanhood.
On a recent trip to Australia, I had many raw, open conversations of this flavor with Aussie moms—many eager to make sense of how different the experience of women’s healthcare is in America. I noticed, too, a different attitude towards moms, babies and families more broadly in the public sphere. Local pubs are filled with newborns strapped to moms and dads alike. At every coffee shop, toddlers happily sip on frothy "babycinos." Families seemed to belong in public spaces in a way that feels all too rare to me in the U.S.
Meanwhile, back at home, an unsettling irony was unfolding: a growing pronatalist movement urging Americans to have more babies, set against the backdrop of a harrowing maternal health crisis.
In the short ten days I was gone, HHS abruptly slashed funding for the landmark Women’s Health Initiative—only to restore it days later after public backlash. Our self-described “fertilization president” floated a $5,000 “baby bonus,” all while federal efforts to gut Medicaid—the single largest payer of maternity and newborn care in the U.S.—continue to escalate.
We can’t ignore the contradiction: we’re urging women to have more babies while failing to make motherhood safe, supported or affordable.
Countries like Australia, where maternal mortality rates are five times lower than the U.S., offer a glimpse of an alternative: not a utopia, but a model that’s both attainable, sustainable—and I believe, within reach.
In this piece, I unpack:
The data: A side-by-side look at U.S. vs. Australian maternal health outcomes
The drivers: The care model and policies behind the stark differences
The opportunity: A skeleton proposal for it would take—and cost—to bring an Australian-style maternity model to the U.S.
Here’s the spoiler: Unlike so many problems of our time, improving maternal health is solvable. It doesn’t require a breakthrough technology or a moonshot. It just requires the will to build a system that puts women and families first.
A U.S. vs. Australia data deep dive reveals a stark maternal health divide
It's well-documented that the U.S. has the highest maternal mortality rate among developed nations, with particularly harrowing outcomes for Black women. Despite spending more per pregnancy than nearly any other country, our outcomes lag across every quality and cost metric—most critically, a woman’s ability to survive her pregnancy.
Graphs like this one from the Commonwealth Fund illustrate this glaring disparity:

Rather than refresh familiar headlines, I wanted to take a closer look at how the U.S. compares to one country, Australia. Why Australia? My personal travel escapades aside, it’s a similarly high-income and well-educated country, but one that offers more social support than the U.S.—without sitting on the far end of the social welfare spectrum a la Sweden.
Unlike the Nordic countries—whose social safety nets can feel politically or culturally out of reach for many Americans—Australia offers a middle path: more public investment than the U.S., but without the perception of a “socialist” system. It’s not a utopian outlier, and instead provides us a plausible blueprint for improving maternal health in the U.S. at a time of national (and dare I say, bipartisan) interest. Let’s dig in.
Maternal mortality:
In 2022, the U.S. maternal mortality rate was 22.3 deaths per 100,000 live births—a decrease from 32.9 in 2021 (peak-Covid), but still significantly higher than our peers. In contrast, Australia reported a maternal mortality rate of 4.8 deaths per 100,000 women—nearly 5X times lower than the U.S.

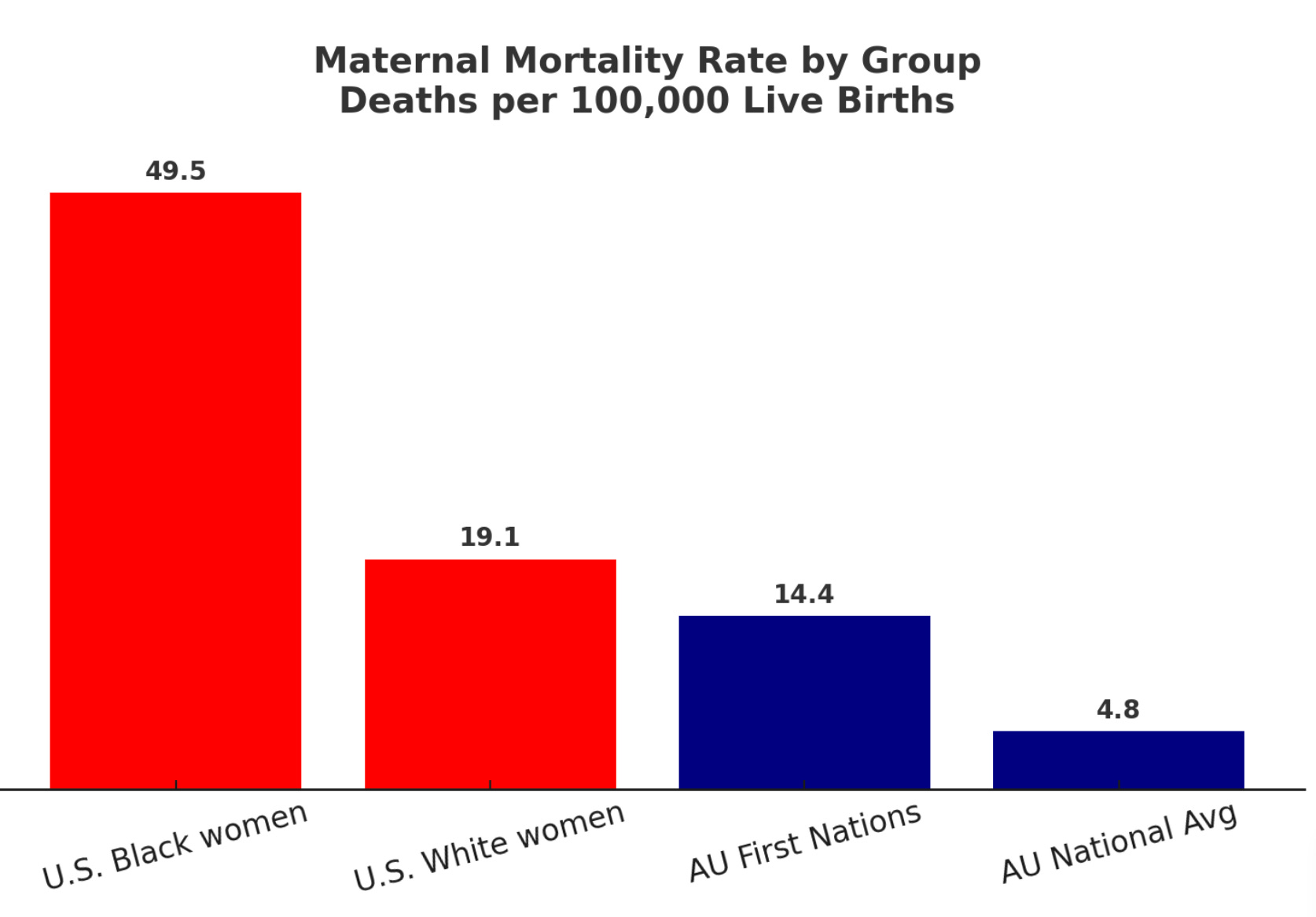
Racial and ethnic disparities:
Both the U.S. and Australia report stark disparities in maternal outcomes among racially and ethnically marginalized groups. In the U.S., the largest gap is between White women and Black women, who face dramatically worse outcomes than any other racial group. In Australia, the most significant disparity—and the focus of policy attention—is between White women and Aboriginal and Torres Strait Islander women (often referred to as First Nations women).
Note: Australia does not currently report maternal mortality rates disaggregated by ethnicity for non-First Nations women. The national average is used here as the best available comparison point. In contrast, the U.S. reports maternal mortality rates by race, enabling direct comparisons between Black and White women.
In the United States:
Black women face a maternal mortality rate of 49.5 deaths per 100,000 live births — more than double the national average, and over 2.5x the rate for White women (2022).
Native American and Alaska Native women also experience significantly elevated risk and mortality, though comprehensive national data remains limited and is therefore not reflected in the graph above.
In Australia:
Though Australia is more racially and ethnically homogeneous than the U.S., disparities persist—particularly for Aboriginal and Torres Strait Islander women (AU First Nations).
Between 2013 and 2022, the maternal mortality rate for First Nations women was 14.4 deaths per 100,000 births—nearly 3X the national average.
While the disparities in each country stem from distinct histories and systems—and shouldn’t be compared “apples to apples”—they reveal a common truth: structural inequity drives maternal health gaps. The specifics vary by population and context, but comparing the scale of these disparities helps illuminate how public policy and care delivery models can either close those gaps—or deepen them.
→ Key takeaway: even accounting for within-country inequities, Australia’s worst maternal health outcomes are still significantly better than outcomes for American women of any race. It’s a sobering reflection of what happens when access to care, postpartum support, and public investment diverge.
Other key quality metrics + drivers of outcomes:
Maternal mortality grabs headlines, but to understand what’s driving outcomes—and what can be done to improve them—we have to look deeper. From my experience designing care models at Tia and debating these very questions with leading payors and health systems, I’ve learned that a handful of metrics are consistently used to measure and manage maternity care across the prenatal, birth, and postpartum continuum. You can think of these as the “leading indicators” most predictive of outcomes and cost:
Engagement in early prenatal care
Preterm birth and C-section rates
Engagement in postpartum care
Provider ratios and access
Maternal age
Taken together, these metrics offer a more dimensional view of maternal health—not just whether mothers survive, but what kind of care they receive along the way. Interestingly (and perhaps not surprisingly), Australia outperforms the U.S. on every single one—except C-section rate.

We’ll dig into these dynamics further in the care model deep dive, but a few initial callouts:
→ Maternal Age: If you're thinking the U.S. has worse maternal outcomes because American women are waiting longer to have children, think again. Australian women, on average, begin their motherhood journeys two years later than women in the U.S., and yet they experience far better outcomes across the board. Delaying motherhood isn’t the primary issue; the system is.
→ Preterm birth rate: Arguably the most important quality metric to watch. The U.S. has a significantly higher rate of preterm births, which not only impacts the health of both mother and baby, but drives enormous cost due to the NICU stays that often follow. Unlike C-sections—which are rising globally and partly influenced by patient and provider preferences—preterm birth, in my view, is a cleaner proxy for systemic issues. It reflects the downstream effects of poor access to primary and prenatal care, rising maternal stress, unmanaged chronic conditions, and other risk factors that make pregnancy more complex from the start.
→ Provider ratios: When you combine OB/GYNs and midwives, the U.S. has just 16 providers per 1,000 live births. Australia has 78. That’s nearly a 5x difference in perinatal workforce capacity. The U.S. system is not just OB-centric—it’s severely understaffed and fragmented—a problem that’s only worsening post-Dobbs, as more OB/GYNs leave restricted states or exit the field altogether, and enrollment in OB/GYN residency programs continue to decline. It’s a travesty to witness entire U.S. counties turn into “maternity deserts” without a single practicing women’s health provider.
Putting aside the midwife vs. OB debate for a moment, one thing is clear: if we want to increase the birth rate, we need to fix the women’s health workforce shortage.
→ C-Section rate: This is the one area where the U.S. “outperforms” Australia. This surprised me given the predominance of Australia’s midwife-led model (for those unfamiliar, only OBs—or surgeons—perform C-sections). I am not an expert, but my best guess is that this difference is driven by higher rates of elective C-sections in Australia’s private system (where patients choose OBs directly), or necessary escalations from midwife to OB care in the public system. If any Aussie readers are here, I’d love your take.
That said, C-section rate is a hotly debated quality metric—it’s rising around the world, often due to non-clinical factors (just search “scheduled C” on TikTok to get a consumer POV). While C-sections do influence outcomes and costs, they’re a smaller cost driver than preterm birth. So for the purposes of this piece, I will focus more closely on preterm birth and the care model factors behind it.
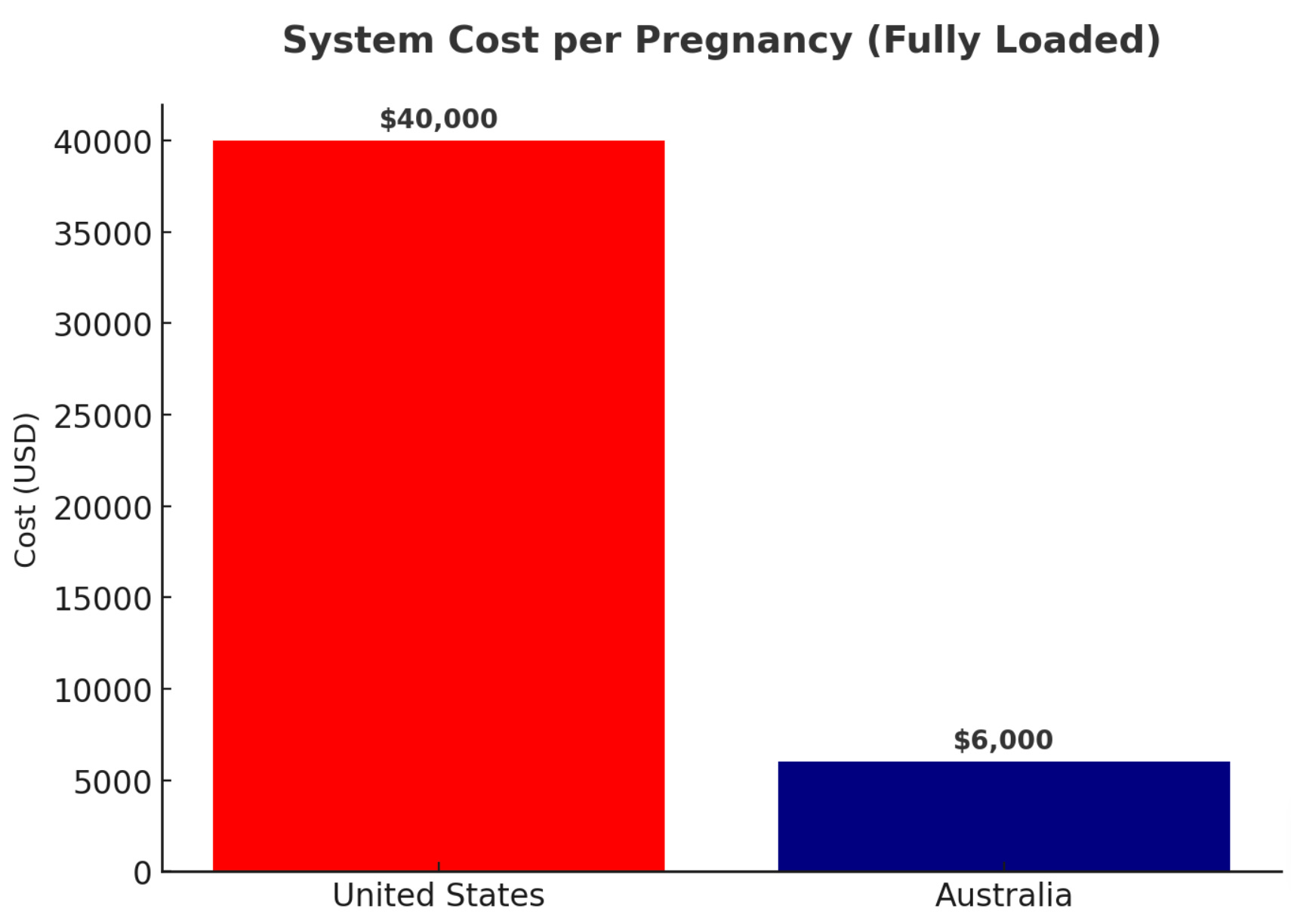
The final kicker: cost
In the U.S., the healthcare system spends an estimated $30,000 to $50,000 per pregnancy when accounting for prenatal care, delivery, and complications like NICU stays. In Australia, that number is closer to $5,000 to $7,500 USD—a fraction of the cost and with far better outcomes.
The difference isn’t just in what we spend—it’s what’s we get for those dollars, both in services and outcomes. Australia’s public system covers the full arc: prenatal visits, ultrasounds, labor and delivery, postpartum nurse home visits, mental health screening, and enrollment in child health checkups. The U.S. system, by contrast, often ends at hospital discharge—though some Medicaid expansion states, like California, offer more expansive postpartum support. What’s more, care for mom and baby is split across separate payment models, despite obvious clinical connections—a source of intense policy debate that makes efforts to reduce costly outcomes like NICU stays really challenging.
If you’re wondering about the cost to women themselves, it’s equally stark: in Australia’s public system, most women pay nothing out of pocket; in the U.S., even with insurance, women pay an average of ~$2,800 per pregnancy—and much more if they experience complications, are underinsured or opt for additional support services like doulas, lactation consultants, or mental health care. Every Aussie woman I spoke with looked genuinely stunned when I mentioned the prospect of receiving an itemized bill after giving birth.
Regardless of what you think about government-sponsored healthcare, the point is we are paying more and getting less. Whether the government or individual families are paying, let’s at least ensure we’re getting a safe— and preferably, a joy-filled—experience in return.
Four pillars of Australia’s higher quality, lower cost maternity model
The data is clear: across nearly every quality and cost metric, Australia outperforms the U.S. on maternal health by orders of magnitude. What’s the secret? It’s not AI or some revolutionary medical breakthrough. It’s something far simpler—a set of foundational, patient-centered practices made accessible to everyone through smart, national policy.
The more I spoke with Aussie moms, the more curious I became about the model behind their personal stories. A closer look revealed four pillars at the heart of the system:
Team-based, midwife-led care
Robust postpartum support
Universal coverage
Integrated paid family leave
Let’s unpack how each of these pillars actually works—and what it would take to bring them to life in the U.S.
1. Team-Based, Midwife Led Care
In Australia, most women receive care throughout their pregnancy, birth, and postpartum journey from a midwife or care team that includes midwives and nurses with OBs as “backup.” If you want to see an OB throughout your pregnancy, you need to “pay up” in the private care system (more on this below). This model has been shown to deliver better outcomes in Australia and in many countries around the world—especially for low-risk pregnancies that don’t require the higher-cost, higher-intervention approach of a surgeon. OBs are still a critical part of the system, but they’re brought in when needed, not by default.
Midwifery is arguably the oldest form of healthcare on the planet—women supporting women through birth long before hospitals or modern medicine existed. And yet, despite centuries of evidence and global adoption, midwives attend only about 10% of births in the U.S. OBs are still the default provider, even when a lower-intervention model would better match the patient’s needs and risk profile.
For those unfamiliar, midwives are licensed, highly trained clinicians who provide comprehensive, whole-person care—not just during labor and delivery, but across prenatal visits, birth planning, postpartum recovery, lactation support, and even mental health. They’re experts in physiologic birth and patient education, and they bring a relational, often trauma-informed approach that many birthing people are actively seeking. It’s not surprising that a growing number of women in the U.S.—especially younger, healthier patients—say they want a midwife-managed pregnancy, or a hybrid option with a midwife and OB working together. Not to mention, midwives are less expensive than OBs!
But access is a different story. State-by-state regulatory restrictions and hospital credentialing rules often limit midwives’ ability to practice at the top of their license. And in rural areas or maternity care deserts—where OBs are disappearing post-Dobbs and hospitals are closing entire L&D (labor and delivery) units—midwives could be a lifeline. Yet in many states, they’re legally barred from filling the gap.
Fortunately, a wave of innovative U.S. startups are building new models to meet this demand. Women’s health startups like Oula, Millie and Quilted Health are making collaborative midwife/OB models more accessible here in the U.S.—offering an alternative for women who want a lower-intervention experience without committing to a home birth in a bathtub (there’s a big spectrum!).
And they have the outcomes to show for it. Take Oula, for example: with 3 clinics in New York and one more opening soon in Connecticut, they combine midwives and OB/GYNs into an integrated model that spans prenatal, delivery, and postpartum care. Across their 2,400 births to date, they've shown a 30% lower c-section rate and 50% lower preterm birth rate, resulting in more than $6.5 million in direct medical cost savings.
We have the proof—in countries around the world and in frontier startups here at home. We don’t need to reinvent care. We just need to back what already works—and what more and more women are asking for.
2. Robust Postpartum Support
In Australia, postpartum care isn’t an afterthought—it’s a core part of the maternity care continuum. What I found most striking is the mental model: care is brought to the mother, not the other way around.
Within days of leaving the hospital, every new mom receives an at-home visit from a trained Child and Family Health Nurse—someone who checks in on the mother’s physical healing, the baby’s development, breastfeeding, sleep, mental health, and more. These visits are opt-out, not opt-in, and the frequency scales based on the family’s needs.
Imagine this: instead of a generic email or a transactional text from your patient portal, an actual human being shows up at your door within 48 hours of returning home—not to collect a copay, but to check on you. Not just to weigh the baby, but to ask how you’re sleeping, how your stitches are healing, whether you're feeling like yourself, and if you need help with breastfeeding. And then, you’re invited into a free, government-funded mothers’ group in your neighborhood—a space for peer connection, parenting education, and community that continues well beyond the first few weeks.
Every Aussie mom I spoke with cited these nurse visits and mothers’ groups as essential life-lines—improving their health, their baby’s and providing an essential source of connection and delight amidst a lonely and overwhelming journey.
Contrast that with the U.S. where pregnancy care often ends with delivery—despite two-thirds of pregnancy-related deaths happening after a woman leaves the hospital. Putting aside emotional well-being for a moment, this graph from Commonwealth Fund speaks to the gravity of the problem:

If an American mother is lucky, she’ll have one 6-week postpartum check in at her OB’s office—often little more than a box-check depression screening. It’s no surprise that nearly 40% of women never attend it, and fewer than half see a primary care provider within a year of giving birth. There’s no home visit. No structured follow-up. No continuity of care.
Some startups like Maven, Pomelo Care and Cayaba Care are working to fill this gap with “wraparound” offerings—designed to complement, not replace, your OB or midwife, with an extra focus on postpartum. Maven’s employer-sponsored platform spans the full reproductive journey from fertility through postpartum, acting as a broker that connects women with an array of virtual services from sleep coaches to lactation consultants. Pomelo focuses on clinically-integrated care for high-risk moms and babies, working directly with payors to reduce complications and NICU stays. Cayaba’s model is anchored on giving every patient a dedicated “Maternity Navigator’ to support a patient 24/7 during pregnancy and for a full year after delivery.
While venture-backed real-world models are harder to come by, Mahmee has built a hybrid model that centers the distinct needs of Black women. They combine virtual support with in-person services including doulas and in-home lactation counseling, largely in the LA area.
Some argue that while real-world care models may be impactful, they are harder to scale. I say: what’s the blocker? We already deliver home-based care at scale for elderly patients (paid for by Medicare), for post-surgical recovery, and even for frivolous hangover IV drips.
Why not for new moms?
3. Universal Coverage
All of this care is made possible by universal health coverage. Under Australia’s public Medicare system, the full arc of maternity care—from prenatal visits and ultrasounds to hospital delivery and home postpartum support—is covered, regardless of income. Private care is available for those who want it, but the public option delivers excellent outcomes and isn’t necessarily seen as superior. In fact, some of the women I spoke with mentioned actually opting out of private care and into public care for their pregnancies in order to access desirable offerings like midwife-led, group-based prenatal visits (known as “centering”) that are only available through the public system.
In the U.S., coverage is fragmented and expensive for all parties involved—women, employers and the government (aka taxpayers). Families live in fear of being crippled by a surprise medical bill post-delivery, as do self-insured employers and state Medicaid programs who have to stomach the notorious “million dollar babies” due to high preterm birth rights and sky-high NICU costs. Everyone is paying more, and still getting less.
So, what do we do about it?
Let’s be realistic: a “Medicare for all” overhaul isn’t happening anytime soon in the U.S. under any administration. But, I'm a firm believer that we don’t need to solve the entire system to start making progress.
What if, in this moment of renewed political attention on fertility and family-building, we carved out pregnancy and childbirth as a federally guaranteed benefit?
There’s precedent for this. The U.S. government has created carve-outs before—fully funding care for specific, high-stakes conditions when the moral and medical case was clear enough:
End-Stage Renal Disease (ESRD): Since 1972, all Americans with ESRD—regardless of age—are eligible for Medicare coverage for dialysis and kidney transplants. It’s the only condition-based path to guaranteed coverage in the U.S.
ALS (Lou Gehrig’s Disease): In 2020, Congress eliminated the standard five-month waiting period for people diagnosed with ALS to accelerate coverage—recognizing the urgency and burden of the disease.
These carve-outs prove what’s possible when we treat healthcare access as a priority, not a privilege. We already have a playbook for federally funded care when the stakes are high. What’s higher stakes than bringing a child into the world and keeping the mother alive to raise them? This isn’t about ideology. It’s about creating a common-sense, evidence-based floor of support for moms, babies and families.
4. Paid Leave
Underpinning Australia’s maternity model is another critical piece: guaranteed paid parental leave. In the U.S., we tend to treat maternity care and paid leave as separate conversations—but they are inextricably linked, both in principle and in practice.
In Australia, new parents are entitled to 20 weeks of paid leave at the national minimum wage, funded by the government. This leave can be shared between parents or taken flexibly over time and many employers top it up with additional pay or time off. The majority of women I spoke with—many in knowledge-economy jobs—took 6 to 12 months off through a combination of paid and unpaid leave, then eased back in 3-4 days a week before ramping up to full-time. It's not perfect, but it’s flexible and gives parents options to choose what works best for their family. Most importantly, it sends a clear message: recovering from birth and bonding with a new baby is a public priority, not a personal luxury.
In the U.S., the picture couldn’t be more different.
There’s no federal paid leave policy—only a patchwork promise of 12 weeks of unpaid time off under the Family and Medical Leave Act (FMLA), which only covers about 56% of workers. Many new moms are forced to return to work just 2–6 weeks postpartum—often still bleeding, in pain, and utterly exhausted—because they can’t afford not to.
And remember the Commonwealth Fund chart above? Two-thirds of U.S. maternal-related deaths occur in the postpartum period—many well after six weeks, just as most American moms are returning to work. The data is unignorable; this is abysmal public health policy.
While some large employers with deep pockets offer more generous leave, access varies wildly by geography, job type, and race. Only 24% of private-sector workers have access to any paid family leave at all.
As someone who ran a company with 400+ employees—most of them in their peak reproductive years—I can tell you firsthand: putting the onus on employers to solve this problem on their own is financially untenable. Outside of companies like Google or Meta, most small and mid-sized businesses simply can’t afford to fully fund extended leave, no matter how much they care. This isn’t a matter of values—it’s a matter of economics. The government has to step in.
The good news? Paid leave is one of the few areas of real bipartisan support.
Red and blue states alike—from California to Oklahoma—have piloted successful paid leave programs. Poll after poll shows broad support across party lines. Even some conservatives have framed paid leave as a pro-family, pro-baby policy.
In a time of unprecedented division and political polarization, paid leave is a rare opportunity for common ground. Let’s seize it—and pass a baseline federal policy that gives families the time they need to recover from birth and care for their newborns.
Whatever your political views may be, surely we can agree on this: a healthy start for moms and babies should be foundational to making America both healthy—and great—again.
But wait… how can we afford it?
If you’ve made it this far, you might be thinking: “You’ve lost your mind. Have you seen the headlines? DOGE is looking to slash three trillion in spending, and you want to expand maternity care and paid family leave?”
Fair. But I like to think of myself as a pragmatic optimist—so here’s a back-of-the-envelope math that shows how this could be a smart cost-savings play, not a bloated welfare program.
Step 1: Breaking down what we spend today
Let’s start with the baseline: the U.S. spends ~$144 billion per year on maternity care for ~3.6 million births—and still has the worst maternal health outcomes in the developed world.
So, who’s footing the bill?
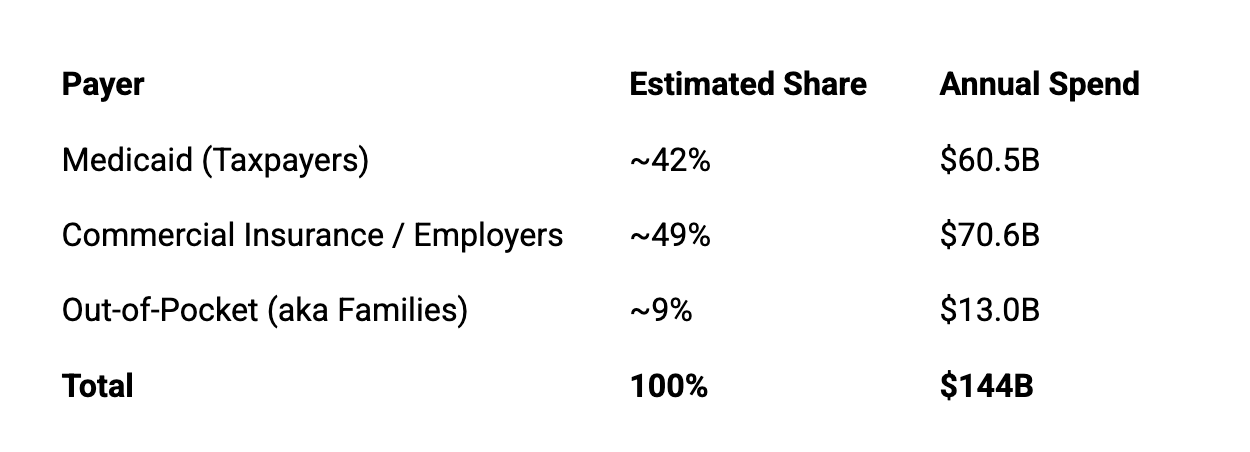
→ Takeaway: We’re already spending a fortune here (and failing families while we’re at it); we’re paying for it through taxes, skyrocketing insurance premiums, and personal debt. Can we afford not to change our model?
Step 2: Estimating costs to implement the Australian model
For simplicity, let’s take the core tenets of the Australian system as-is—midwife-led care with OBs as backup, postpartum home visits, and community-based follow-up—and apply them to the current U.S. birth volume.
Estimated cost per pregnancy in AU (including NICU): ~$7,500 USD (high end)
3.6 million U.S births/year × $7,500 = $27B/year
→ Takeaway: We could offer every pregnant woman in America full-spectrum, evidence-based maternity care for less than half of what we’re currently spending—and get far better outcomes. (more on that math in Step 4.)
Step 3: Add 20 weeks of paid leave
Now let’s factor in paid parental leave as a guaranteed, federally-funded baseline, just like in Australia.
Again, for the purposes of this exercise, let’s assume the U.S. adopts the same 20-week policy, paid at the federal minimum wage. In Australia, the minimum wage is $23.23/hour AUD—or about $15.50 USD. In the U.S., the federal minimum wage is currently $7.25/hour—I’ll save my rant on that for another day, but it’s important to mention the delta for obvious reasons.
20 weeks × 40 hours/week × $7.25/hour = $5,800 per family
$5,800 × 3.6 million births/year = $20.9B/year
Let’s call this what it is: a floor, not a ceiling. Some employers would likely top it up (as they do in Australia). Some parents would take unpaid time on top. This is intended to be a federally guaranteed starting point.
→ Takeaway: Funding this paid leave policy at ~$5,800 per baby is more or less in line with President Trump’s proposed $5K “baby bonus.” But, structured as paid leave, it would have far more impact:
It gives families flexibility to decide who goes back to work when—based on varying income levels, recovery factors, caregiving dynamics, and a whole bunch of other things that individual families should decide, not the government.
It offers employers and states clear legislative rails to build on top of—whether by bridging to a higher minimum wage (currently $16 per hour in California as an example) or filling in the gap between minimum wage and a parent’s full salary.
Same cost. Greater impact. Real infrastructure for long-term change.
Step 4: Bringing the pieces together:
What’s the final bill—and what could we save? Let’s add it all up:
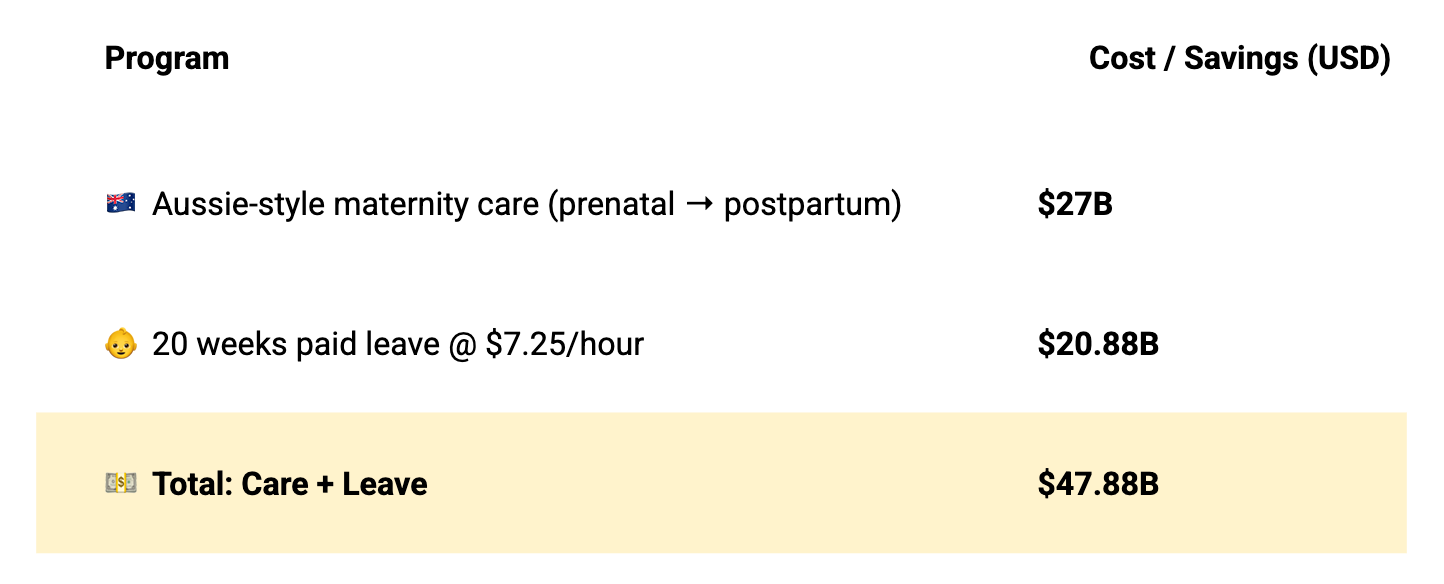
~$48B might sound like a big number—but remember, we currently spend $144B per year on maternity care in the U.S., with at least $60B of that stemming from taxpayer-funded Medicaid alone.
Here’s the catch: whether this new price tag holds depends on how substantially we improve outcomes—particularly reducing preterm births and NICU stays, which drive a large portion of U.S. maternity costs. But, we know the Aussie model works to improve this exact metric (amongst others): more proactive care, delivered by lower-cost, lower-intervention providers, leads to fewer complications and better outcomes.
Even if we get 50% of the outcome improvements, this Aussie-style maternity model would still cost far less than what we spend today—all while saving tens of thousands of lives saved.
→ Final Takeaway: Instead of spending $144B reacting to poor outcomes, we could fund comprehensive maternity care, 20 weeks of paid leave, and still save billions—all while making motherhood safer, more equitable, and more humane.
Zooming way back out
The goal of this exercise isn’t to suggest we actually copy-paste Australia’s model line by line. It’s to show that a better, safer, more humane system is within reach—one that builds on what already exists and leverage best practices proven both here and abroad.
If you take away just a few things away, let it be these:
We know how to improve maternal health outcomes. We don’t need AI or surgical robots to fix maternity care, or some not-yet-invented technology. The solutions are ancient and well-proven: midwives, home visits, paid time to heal. It’s not an “if” problem — it’s a will problem.
Let’s not miss the forest for the trees. In many women’s health circles I’m part of, I see well-intentioned people get stuck in the weeds. Divisive debates over the optimal midwife to OB ratio, or whether we prioritize doulas vs at-home nurse visits often dominate at the expense of broader action. These are valid questions, but over-analysis can become its own form of inertia, slowing down progress when we have proven practices ready to scale.
Progress is better than perfect. I’ll be honest: $7.25/hour is a drop in the bucket— and probably insulting to many readers here. It’s nowhere near enough to reflect the value of new parenthood or caregiving, let alone a livable wage for actual “workplace” work. But, as a federal floor that states and employers can build on top of? It would provide a meaningful step forward—and a far cry better than today’s reality of zero guaranteed pay and zero protected time.
We can improve outcomes and reduce costs at the same time. At a time of national reckoning on spending and debt, there is strong data to support that investing in women’s health would yield strong ROI in both dollars and lives. This isn’t a utopian fantasy. It's a fiscally responsible public health strategy.
Intentions don’t have to be pure to be useful. Some readers may bristle at the motivations behind certain “pro-family” proposals in today’s political landscape. I get it. But if those policies create bipartisan momentum to improve women’s lives? Let’s make progress—and keep pushing for more.
I don’t want to write—or read—another gut-wrenching headline about a mother dying from something preventable. We have the data. We have viable models we can back and scale. And just maybe, we have growing political will. Let’s not waste it. The stakes have never been higher.
A special thanks to for reading drafts of this piece!
I’d love to hear from you ❤️
This piece was an experiment—for me, it’s both more personal and more data than usual. I’m trying to explore how we move beyond headlines and into real conversation, even when the solutions aren’t always clear. Because the truth is: problems of this scale are bigger than any one of us.
I don’t claim to have all the answers—but I do believe that sharing observations, personal experience, and data can help spark something meaningful. If you’ve experienced maternity care in the U.S., Australia, or anywhere else, I’d be grateful to hear your story.
Drop a comment below, send me an email, or forward this to someone who might want to join the conversation.
Well researched and written. Carolyn, you have provided data to support the value of crafting a plan for the US as well as negating likely objections. Now I’m pondering where your research might get serious audience.
The time is now to fix the system- care for women after their reproductive years is not any better. Thank you for writing such a great article!